
StrongMinds – Comprehensive Summary
Last updated: December, 2024
Problem
Depression is strongly linked with lower subjective wellbeing (Clark et al., 2017), but mental health services are significantly underfunded in low- and middle-income countries (LMICs)1 Mental and addictive disorders form between 7% and 13% of the global disease burden (Vigo et al., 2019; IHME, 2021), depression and anxiety being the most common (Ferrari et al., 2022) and their relative share has grown in recent years (Rehm & Shield, 2019). However, these disorders only receive 1% of governmental health budgets in LMICs (Vigo et al., 2019) and 0.3% of health-directed international assistance (Liese et al., 2019).. In LMICs, only 13.7% of people with mental illness receive treatment (Evans-Lack et al., 2018). This figure is 10.8% for anxiety, of which 2.3% is considered “potentially adequate” (Alonso et al., 2018), and 8% for depression (3% adequately treated; Moitra et al., 2022). Together, these facts suggest that improving mental health is a severely neglected problem.
Intervention
Group interpersonal therapy (g-IPT) treats depression by increasing social support, decreasing the stress of social interactions, and improving communication skills. When g-IPT is facilitated by community members who receive a few weeks of training – instead of psychotherapists – it is called “task-shifted”. Task-shifted g-IPT is the intervention that the WHO recommends for cost-effectively tackling mental health in LMICs.
Organisation
StrongMinds provides g-IPT in Uganda and Zambia through several programmes. The core programme is task-shifted g-IPT delivered in person in 90-minute weekly sessions over multiple weeks. Historically, the programme was delivered over 12 weeks, but StrongMinds has reduced this to 6 weeks with more focused content2Individuals are divided into groups depending on which coping strategy appears most relevant to their case: increasing social support, decreasing the stress of social interactions, or improving communication skills (StrongMinds personal communication, 2023). The official programme is sometimes followed by a longer unofficial phase where the groups continue to meet and support one another without the presence of an official facilitator (StrongMinds, 2017).. In recent years, StrongMinds has largely shifted away from directly deploying its programmes to training non-government and government organisations to deliver g-IPT3StrongMinds primarily provides psychotherapy through partner organisations (78%). StrongMinds (and partners) mainly operate in Uganda (70%) and Zambia (30%). The partners StrongMinds works with are 70% government affiliated workers: community health workers and teachers. The remaining 30% of the partnerships are through a variety of NGOs.. Clients often continue meeting in their groups after the therapy sessions have ended.
Evaluation
Methods
To estimate the impact of StrongMinds, we combined general evidence of the impact of psychotherapy on subjective wellbeing in low- and middle-income countries with evidence directly evaluating the impact of StrongMinds’ program: 1 RCT related to StrongMinds4This is the Baird et al. (2024) RCT. We discuss its limited relevance in the FAQs. and StrongMinds’ monitoring and evaluating pre-post data.
For the general evidence we first conducted a systematic review to gather general evidence on the impact of psychotherapy5We defined psychotherapy as an intervention with a structured, face-to-face talk format, grounded in an accepted and plausible psychological theory, and delivered by someone with some level of training. on subjective wellbeing in low- and middle-income countries. After excluding outliers and ‘high risk of bias’ studies, we collected 84 RCTs with a sample of 25,363 unique participants.
We then estimated the effects in each source using a meta-analysis6For each psychotherapy intervention, we extract every follow-up over time for every outcome measure that fits our inclusion criteria. This means that there is dependency (i.e., non-independence) between the effect sizes within an intervention between outcomes collected for a certain timepoint, and between timepoints for a given intervention. We select a 3-level (random effects) model to account for this dependency.. We measured the effect from each study using Hedges’ g standardised mean differences, which is interpreted as the improvement in standard deviations7Our preferred measures of wellbeing are self-reported life satisfaction or happiness, but many of the studies we found used measures of affective mental health (MHa; i.e., depression, general anxiety, or general distress). Standard deviations of MHa were converted to standard deviations of wellbeing using a 1:1 conversion. See our cost-effectiveness methodology for more detail.. For the pre-post data we use a pseudo-synthetic control method to deal with the lack of control group.
Some studies measured the impact of psychotherapy at different time points. We used this information to estimate the total effect of psychotherapy over time using a meta-regression model8Meta-regressions are like regressions, except the data points (i.e., dependent variables) are effect sizes weighted according to their precision and the explanatory variables are study characteristics. Meta-regressions allow us to explore why effects might differ between studies; in this case, we examine how effects differ depending on the length of time to the follow-up. that assumes the benefits decline at a constant rate over time.
After estimating the total recipient effect over time, we adjust our estimates according to internal validity factors (range restriction, publication bias, etc.) and external validity factors (dosage and other characteristics of the charities).
Then, because improving one person’s mental health can benefit others who are close to that person, we also estimated the spillover effects on household members (i.e., operationalised as a 16% spillover ratio). Thus, the overall household effect includes the estimated impact on recipients and household members over time.
We then calculate a final effect estimate for each charity by combining the three estimates from different evidence sources, using informed subjective weights (i.e., we combine weights based on statistical uncertainty using a Bayesian method with subjective adjustments for harder-to-quantify characteristics).
Finally, we calculate the cost-effectiveness by pairing the estimated effect for each charity with the estimated cost to deliver the intervention.
Impact
We estimate StrongMinds has an overall effect of 1.80 WELLBYs on the individual recipient and their household.
Cost
Based on StrongMinds’ expenditures in 2023, we estimate that it costs StrongMinds $45 to provide treatment to one person.
Cost-effectiveness
The cost-effectiveness of StrongMinds is $25 per WELLBY. This means for every $1,000 donated, the organisation creates 40 WELLBYs.
To quantify the statistical uncertainty in our results, we simulated StrongMinds’ cost-effectiveness thousands of times by varying key parameters9These include: the initial effect and the annual decay rate (which allows for variation in the duration of effects), the household spillover, as well as the household size. to see how the results might differ across a range of reasonable inputs (e.g., Monte Carlo simulations)10Monte Carlo simulations allow us to treat inputs in a cost-effectiveness analysis (CEA) – often merely stated as point estimates – as distribution. Thereby, this allows us to communicate a range of probable values (i.e., uncertainty around the point estimates). See our cost-effectiveness methodology for more detail.. This is illustrated in Figure 1 below.
Figure 1. Density plot of the quantified uncertainty around StrongMinds’ cost-effectiveness
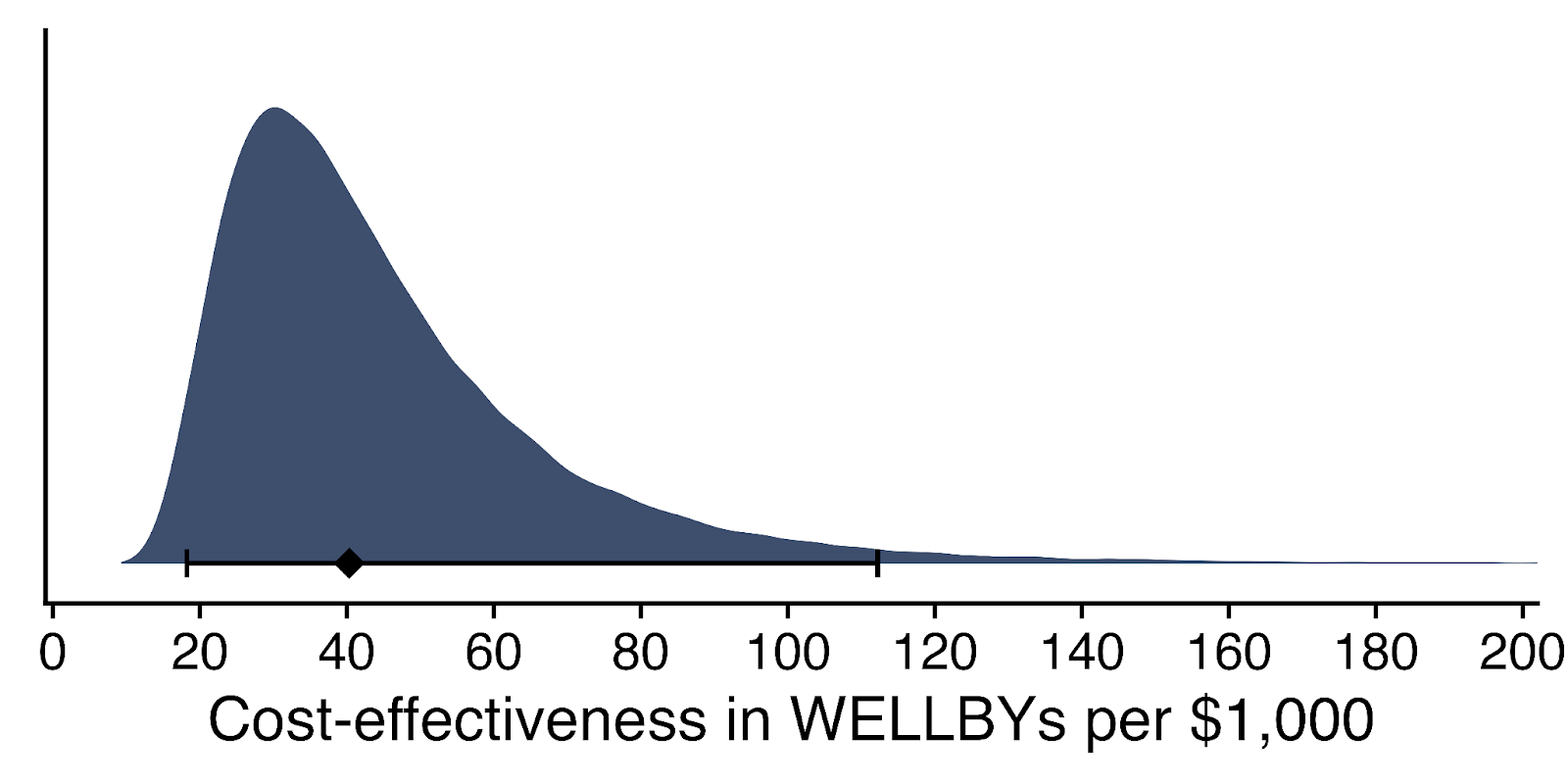
Note. The diamond represents the central estimate of cost-effectiveness. The shaded area is a probability density distribution and the whiskers represent the 95% confidence interval.
Quality of evidence
Our quality of evidence assessment is stringent. We assess quality of evidence according to an adapted version of the ‘GRADE’ criteria, a widely-used and rigorous tool for assessing evidence quality across healthcare and research fields. The GRADE criteria for evidence quality are very stringent, so we expect very few interventions that we evaluate for wellbeing in LMICs (which tend to be less well-studied) will score more than ‘moderate’ on the quality of their evidence. Considering most decisions about charities are made with little-to-no evidence, this is a substantial improvement.
Overall: Low to moderate.
-
General meta-analysis of psychotherapy: moderate. 84 RCTs with low (43%) some (57%) risk of bias (high risk of bias studies were removed). Some inconsistency in effects, limited relevance, and some publication bias (which we adjust for)..
-
SM RCT (Baird et al.): low. 1 RCT with some risk of bias. Issues with relevance (see outstanding uncertainty). Moderate imprecision. Major inconsistency (because cannot verify with one study). No concern about publication bias.
-
SM M&E: very low. Very relevant, but synthetic control provides limited information. Potential for substantial risks of bias.
Depth of our analysis
High. We believe we have reviewed most or all of the relevant available evidence on the topic, and we have completed nearly all (e.g., 90%+) of the analyses we think are useful.
Site visits
Our director, Michael Plant, undertook a day-long site visit to StrongMinds in Uganda. This visit increased our confidence that StrongMinds seems to be reasonably well functioning and making discernable impacts on people’s lives.
Funding need
StrongMinds has a $10 million goal for 2024 with an approximately $3 million gap to fill by the end of December. StrongMinds has raised a total of $3.4 million in pledged funds toward our $11.5 million fundraising goal in 2025. This leaves a fundraising gap of $8.1 million for 2025. The funding will be used primarily to support ongoing work to deliver services to more women. Some funds will also be used to help the organisation scale, and to launch an RCT evaluating its effectiveness.
Conclusion
StrongMinds is one of the most cost-effective and well-evidenced life-improving charities we have evaluated in-depth so far. It is possible that future research could update our evaluation. Overall, we think StrongMinds is a cost-effective way to improve global wellbeing, and is a particularly good fit for donors who value improving lives.
FAQs
- Does psychotherapy actually work?
- Psychotherapy has been shown to be an effective treatment against depression: as good or better than the alternative of drug treatment in many meta-analyses (Cuijpers et al., 2019). Cuijpers et al. (2016) found that interpersonal therapy does not differ in efficacy from other therapy forms, and Cuijpers et al. (2018) supports the idea that psychotherapy is at least as effective in non-Western countries as Western countries. Singla et al. (2017) also found psychological treatments deployed in LMICs to be an effective way to treat depression.
- How does psychotherapy work?
- Psychotherapy works by providing people with a safe space to process their thoughts and feelings, and learn adaptive skills to correct their maladaptive thoughts, emotional processing, behaviours, and social interactions. IPT is a time-limited intervention that focuses on addressing stressful life events and interpersonal challenges, while also helping patients connect with new social supports and improve existing relationships (Weissman et al., 2007; Ravitz & Watson, 2014).
- Is poor mental health only a problem for high-income countries?
- No, the idea of the ‘happy poor’ is not accurate: there are about as many people suffering from mental health problems in LMICs as in HICs (Our World in Data, 2022). Furthermore, treatment for mental health is especially underfunded in LMICs, and even when it is funded, it can vary considerably in quality11For example, it’s still relatively common for people with severe mental illnesses in LMICs to be restrained in solitary confinement and given no other treatment. (Walker et al., 2021).
- What’s the relationship between mental health and poverty?
- Poverty and mental health have a complex bidirectional relationship, where each can worsen each other (Ridley et al., 2020). However, one can be poor without being depressed, and vice-versa. Notably, if mental health problems occur because of maladaptive thoughts, behaviours, and social interactions, then these are causes that can be independent from poverty.
- Does psychotherapy just make people accept poverty?
- No, psychotherapy helps people change maladaptive thoughts, behaviours, and relationships. These can worsen poverty and may not be addressed by alleviating financial burdens – instead, many of these symptoms need specific interventions targeting them, such as psychotherapy. Additionally, mental health interventions – and presumably psychotherapy as well – can improve economic outcomes (Lund et al., 2022)12In fact, the authors find in a quick calculation that mental health interventions are more cost-effective than cash transfers at improving economic outcomes (p. 32)..
- Shouldn’t we just give people cash, so they can decide whether to buy therapy – or something else – for themselves?
- One perspective that’s common among economists is that people are the best judges of what’s good for them. While this may be true in theory, in the real world, people have imperfect information and inadequate options, and other barriers (such as stigma around seeking mental health treatment) may get in the way. The advantage of the WELLBY approach is that, through people’s self-reports, we get evidence on what actually makes a difference to their lives as they live them – not just what they expect would matter. Using these self-reports, our analyses indicate that the effect of providing a depressed person with therapy improves happiness more than giving them, or another non-depressed person, the cash equivalent to the cost of that programme.
- What if people are just saying they feel better because they think it’ll benefit them, or someone else, materially?
- This is a concern about a type of response bias called ‘experimenter-demand effects’, where respondents shift their behaviour in response to their guess of what the study is about. The available evidence we’ve found suggests this is not a major concern, and it likely applies to all research with self-reported outcomes (i.e., it is not specific to psychotherapy). However, the research on the question has been sparse and may not address all concerns, so we’d be interested in seeing more research on this topic. See our more detailed explanation.
- Isn’t Baird et al. (2024) just the most relevant study to use?
-
The Baird et al. trial found a small effect. However, despite the trial taking place in Uganda (where StrongMinds operates) and using a version of StrongMinds’ model, there are several ways in which the Baird et al. study is different from StrongMinds’ actual programme in the field today, which means we cannot generalise from it as much as one might expect. This was the first time StrongMinds had attempted to implement its programme conducted via a new partner. The study involved adolescents receiving therapy from other young people (StrongMinds primarily does therapy for adults led by adults). The facilitators were inexperienced and given insufficient supervision. Attendance was low, with 44% of participants failing to attend any sessions. Furthermore, the long-term data collection overlapped with COVID. These issues are noted by Baird et al. (2024) and/or StrongMinds themselves (StrongMinds, 2024). We give an appreciable, but limited, weight to this source of evidence: 20% of the total, with the remaining 80% coming from the meta-analysis and the monitoring and evaluation data because we think these other sources of evidence are informative as well.
-
- What’s the relationship between HLI and StrongMinds?
- HLI and StrongMinds are completely independent organisations. We are not paid by StrongMinds, and would never accept money to recommend any organisation.
Is your question missing from this list? Contact us at hello@happierlivesinstitute.org.
Our reports so far
We first identified that mental health was a key global priority in our Mental health cause area report. We then evaluated the impact of psychotherapy interventions in the Psychotherapy cost-effectiveness analysis. We identified StrongMinds as a promising charity in the Mental health programme evaluation. We assessed the cost-effectiveness of StrongMinds in the StrongMinds cost-effectiveness analysis. We compared the cost-effectiveness of psychotherapy/StrongMinds to cash transfers/GiveDirectly in our Psychotherapy vs cash transfer comparison. We updated our analysis to include the impact of household spillovers in our household spillover effects report.
In November 2023, we published a substantial update to our psychotherapy analysis and StrongMinds evaluation. This update involved systematically reviewing the literature, updating the evidence for the individual and household effects, correcting for publication bias, and combining the general and charity specific evidence using Bayesian methods. Note that this is a working paper and will be updated over time.
Our director, Michael Plant, undertook a day-long site visit to StrongMinds in Uganda in 2024.
In August 2024 we published an interim update. More importantly, in November 2024, we published another substantial update. We extracted additional studies, double-checked our extraction, conducted double risk of bias analysis, added monitoring and evaluating pre-post data as a source of evidence, updated how we weight the different sources of evidence, expanded our adjustments, expanded the factors that influence our confidence, and used the latest information from StrongMinds.